
- BPH Statistics Worldwide: Global Prevalence
- BPH Diagnosis Statistics and Trends
- BPH Treatment Statistics and Success Rates
- BPH Complications and Hospitalization Statistics
- BPH Mortality Rate Statistics
- Healthcare Costs Statistics on BPH
- Quality of Life Impact Statistics for BPH Patients
- Future Predictions and Research Directions for BPH
- Research Methodology for BPH Statistics
- Conclusion
- Source
BPH is the enlargement of the prostate gland, frequently causing urinary problems because it is located near the urethra.
Benign prostatic hyperplasia (BPH) is a common issue for men globally, most notably as they get older. As the prostate enlarges, it may block urine flow, leading to symptoms such as needing to urinate often, difficulty starting urination, and a weak urine stream. Though it’s not cancerous, BPH can impact a man’s quality of life and need treatment.
In our thorough analysis of BPH statistics, we’ve relied on globally recognized sources like the WHO, peer-reviewed studies, and specialized reports. Reviewed by medical professionals, this data-driven article ensures accuracy and transparency while addressing limitations such as data variation and regional healthcare disparities.
To keep our insights relevant, this page is regularly updated with the latest research, offering readers a clear understanding of key trends and developments in BPH.
Let’s explore the most critical BPH statistics and facts to raise awareness, which can help improve early detection, treatment, and prevention strategies.
BPH Statistics Worldwide: Global Prevalence
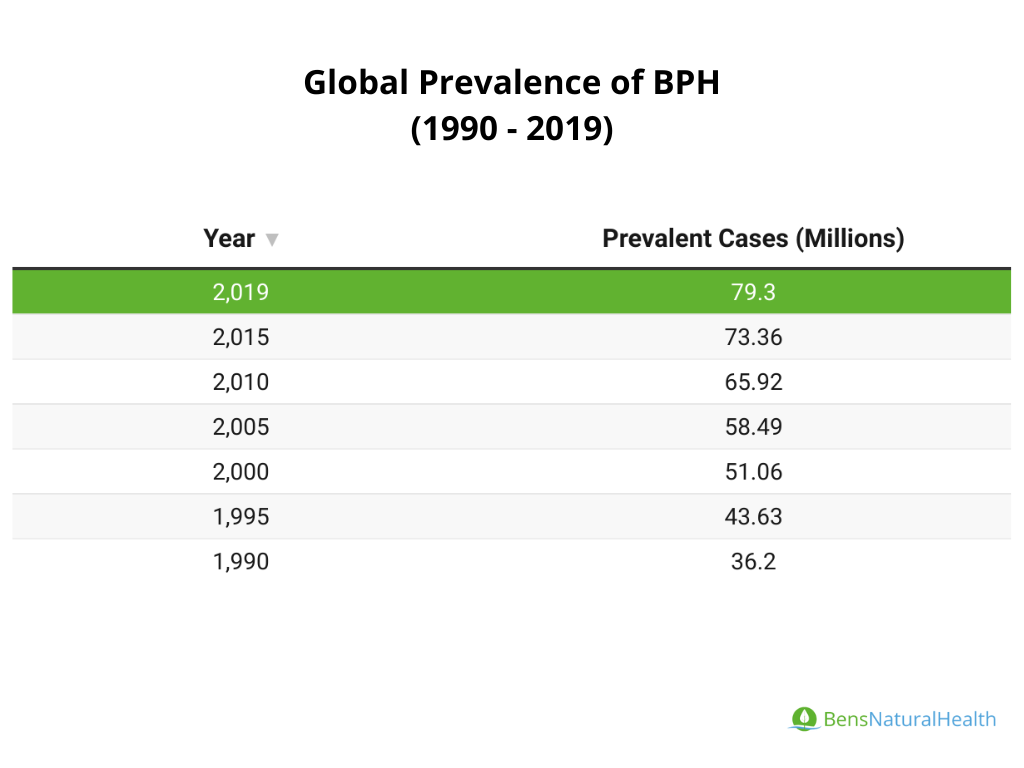
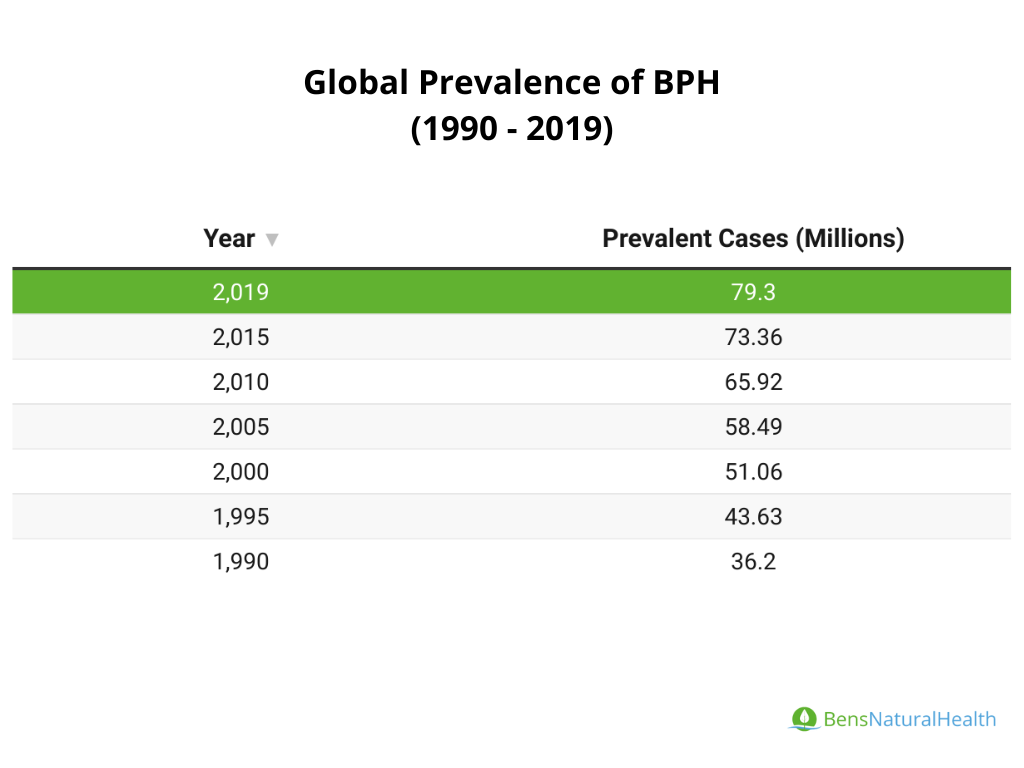
- In 2019, there were approximately 79 million prevalent cases of BPH globally in individuals aged 60 and older. This marks a 119.01% increase since 1990.
- The prevalence rate in 2019 was 16,781 cases per 100,000 population among those aged 60 and over.
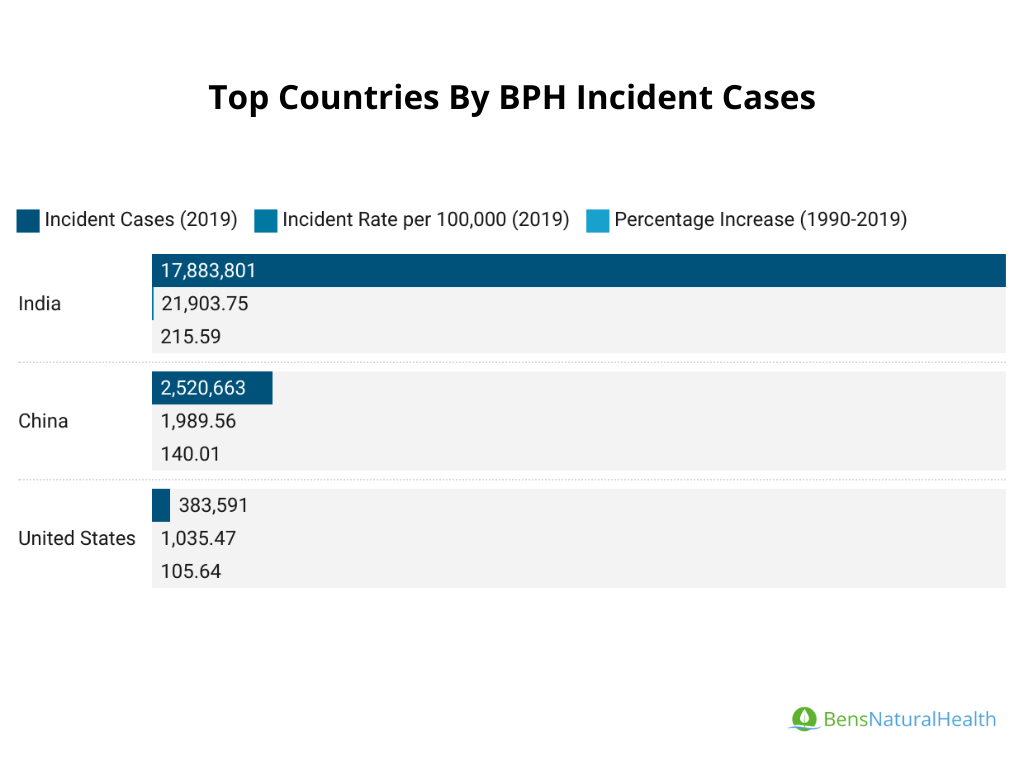
- Countries with the highest number of cases include China, India, and the United States.
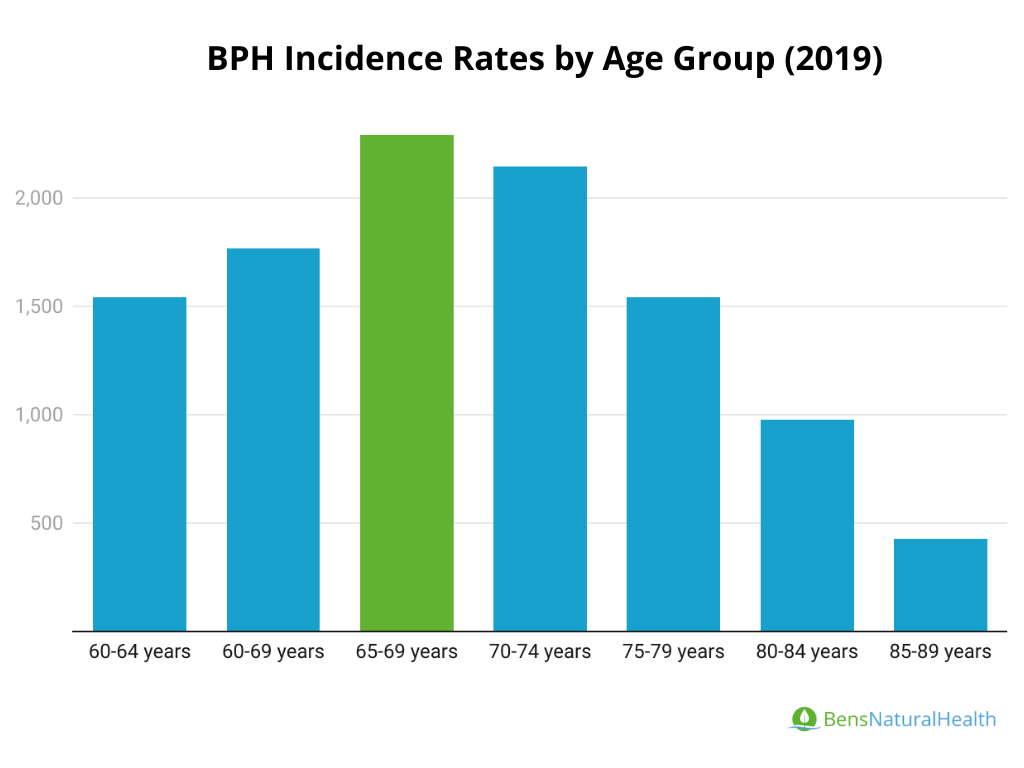
- 65-69 age group had the highest incidence rate, with 2,289.45 cases per 100,000 population.
- Most BPH diagnoses occur in men aged 60 and above, with incidence rates peaking in men over 75.
Percentage of Men with BPH
- Total Global Cases (2019): There were approximately 79 million prevalent cases of BPH globally in men aged 60 and over.
- Age-Specific Prevalence: BPH prevalence increases significantly with age, peaking in the 75-79 age group at 24,324.8 cases per 100,000.
- Regional Prevalence:
- United States: Ranked as one of the top three countries for the burden of BPH cases alongside China and India. Roughly 14 million men in the U.S. are estimated to have BPH. Prevalence among men aged 51–60 is around 50%, rising to 80% among men over 80.
- Europe: Eastern Europe had the highest prevalence rates, with Central Latin America and Andean Latin America also showing high rates.
- Asia: East Asia and South Asia reported the highest numbers of cases by region.
BPH Growth Over the Decades
- Historical Growth (1990–2019): BPH prevalence increased by 119.01% over these three decades.
- Drivers of Growth:
- Population Growth accounted for 94.93% of the increase in BPH cases.
- Aging Population contributed 1.62%.
- Epidemiological Changes accounted for 3.45% of the increase.
- Regions with Notable Growth: Low-middle income regions experienced the most substantial increase at 162.37%.
- Countries with the highest number of cases include China, India, and the United States.
- Regions with the highest prevalence rates were Eastern Europe, Central Latin America, and Andean Latin America.
- The growth in cases was highest in low-middle income regions at 162.37%.
- Disability-Adjusted Life Years (DALYs): In 2019, BPH accounted for over 1.56 million DALYs globally in individuals aged 60 and older, with the highest rates in East Asia, South Asia, and Western Europe.

BPH Incidence Rate Statistics
The incidence of BPH in those aged 60 and over rose over 8.3 million cases globally in 2019, up by 121.22% since 1990.
- Incidence of BPH by Age Group (2019):
- BPH is rare in patients younger than 40 years of age.
- The 65-69 age group had the highest incidence rate, with 2,289.45 newly reported cases per 100,000 population.
- The 75-79 age group had the highest prevalence rate, reaching a total of 24,324.8 cases per 100,000 population.
Genetic, Hereditary, Hormonal BPH Facts
- Men with a family history of BPH have a 2-4 times higher risk of developing the condition.
- Hormonal balance, particularly the ratio of estrogen to testosterone, may contribute to prostate growth. Studies suggest that as men age, the relative increase in estrogen compared to testosterone could stimulate prostatic cell growth, leading to BPH.
BPH Diagnosis Statistics and Trends
BPH commonly presents as lower urinary tract symptoms (LUTS) and generally increases with age.
- Most BPH diagnoses occur in men aged 60 and above, with incidence rates peaking in men over 75.
- BPH symptoms are exceptionally high among elderly males, with some data suggesting a diagnosis peak between ages 58 and 71.

BPH Screening Age: Early Detection Rates
Screening for BPH is often suggested for men over 50, with PSA screening considered for men at higher risk for prostate-related issues.
The American Urological Association (AUA) and similar organizations suggest beginning PSA testing as early as age 40 for men with a family history of prostate issues or African American men who are at higher risk.
BPH Diagnostic Methods Statistics
The DRE (Digital Rectal Exam) remains a foundational diagnostic tool for BPH in both primary and specialized care settings, particularly for assessing prostate size and firmness.
PSA levels are often used to detect prostate enlargement and rule out prostate cancer. Although PSA is a helpful indicator, its use in primary care is more limited than in urology due to cost and resource constraints. Urologists are more likely to use PSA testing and other advanced diagnostics, such as ultrasound or uroflowmetry, to confirm BPH.

BPH Treatment Statistics and Success Rates
Different treatment options are available for BPH, each with its success rates and considerations.
- The global BPH drug market reached $5.34 billion in revenue by 2021.
- Approximately 54% of men with BPH symptoms experience improvement or no worsening without pharmacological treatment, emphasizing the variability in natural progression.
BPH Medication Statistics
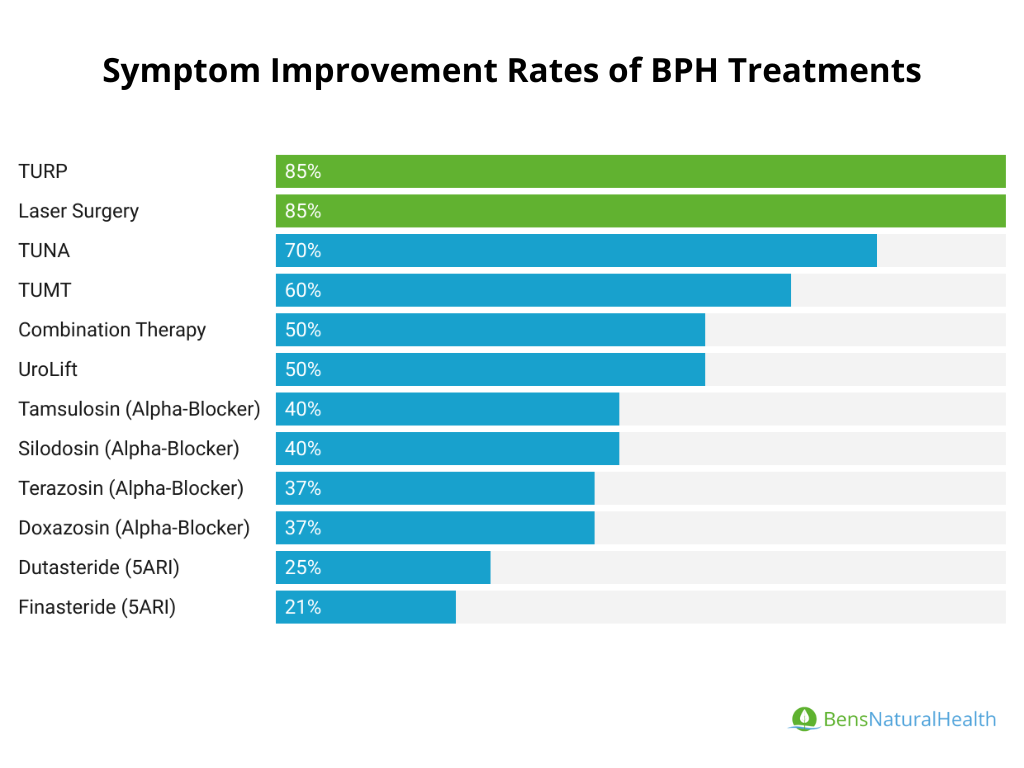
- Terazosin: Improves symptoms by ~37% and peak urinary flow rates by ~22%. It does not reduce prostate size, focusing on symptom relief through smooth muscle relaxation.
- Finasteride: Provides ~20% improvement in symptoms over a year, with sustained prostate size reduction for five years after treatment. Associated with a ~24.8% risk reduction in slow-growing prostate cancer but may increase risks of aggressive cancers.
- Dutasteride: Shrinks prostate size by 25% over two years and reduces acute urinary retention risks by ~57%. Symptom improvement is noted within six months, with an average of ~21% reduction at 24 months.
- Alfuzosin: Improves peak urinary flow rates by ~16-25%, with better tolerability than other alpha-blockers. Like all alpha-blockers, it does not reduce prostate size.
- Combination Therapy: Combining Tamsulosin with Dutasteride addresses both symptoms (via alpha-blockers) and prostate size reduction (via 5-alpha reductase inhibitors). Studies show superior results compared to monotherapy.
- Phosphodiesterase-5 Inhibitors (e.g., Tadalafil): Originally developed for erectile dysfunction, Tadalafil relieves lower urinary tract symptoms (LUTS) associated with BPH. It is particularly effective when combined with alpha-blockers.
- Anticholinergics: Medications like Solifenacin address bladder overactivity symptoms (urgency, frequency) often accompanying BPH.
- Beta-3 Agonists: Drugs such as Mirabegron improve bladder storage capacity with fewer side effects than anticholinergics, making them a preferred choice for managing urinary urgency.

Alpha-Blockers (Selective and Non-Selective): These medications improve symptoms rapidly and are effective for many patients, but they require ongoing use to maintain benefits.
- Selective Alpha-Blockers: Target alpha-1A receptors in the prostate and bladder neck to relax smooth muscle, improving urinary flow.
- Tamsulosin is widely prescribed, showing an improvement of 4-6 points in AUA symptom scores, considered meaningful by patients.
- Silodosin offers higher selectivity but retrograde ejaculation occurs in about 28% of users.
- Non-Selective Alpha-Blockers: Broader action targeting multiple alpha receptors, which also lowers blood pressure.
- Drugs like Terazosin and Doxazosin provide symptom relief for 30-40% of patients, with improvements in peak urinary flow rates of 16-25%. However, these medications often cause dizziness, syncope, and fatigue.
- 5-Alpha Reductase Inhibitors (e.g., Finasteride, Dutasteride): These drugs work by reducing prostate size and have been shown to decrease the need for surgery by 52.9% in some patient groups.
Mechanism and Effectiveness
- Finasteride and dutasteride inhibit the enzyme 5-alpha-reductase, reducing dihydrotestosterone (DHT) levels and shrinking the prostate.
- Finasteride reduces prostate size by ~20% after one year and improves symptoms by ~21% after six months of treatment.
- Dutasteride is more potent and acts faster, reducing prostate size by ~25% over two years.
Side Effects
- Persistent sexual dysfunction, including reduced libido and ejaculatory volume.
- Metabolic side effects such as elevated cholesterol and glucose levels.

Minimally Invasive Treatment Success Rates
Transurethral Microwave Thermotherapy (TUMT):
- TUMT uses microwave energy to destroy excess prostate tissue. It is a single outpatient treatment with a reduced risk of severe complications compared to surgery.
- Success rates vary, with symptom relief observed in approximately 60–80% of patients.
Transurethral Needle Ablation (TUNA):
- This method utilizes radiofrequency energy to ablate targeted prostate tissue.
- Studies report around 70% symptom relief, but higher retreatment rates are noted compared to surgical options.
Prostatic Urethral Lift (UroLift):
- The UroLift system involves placing implants to hold the enlarged prostate away from the urethra, reducing blockage without cutting or removing tissue.
- Clinical studies show UroLift improves IPSS scores by approximately 50%, with a retreatment rate of about 5.4%.
BPH Surgery Success Rate
Transurethral Resection of the Prostate (TURP):
- TURP is considered the gold standard for surgical BPH treatment, involving the removal of obstructive prostate tissue.
- Success rates exceed 80–90%, with significant symptom relief and a retreatment rate of approximately 5.3%.
Laser Surgery:
- Laser procedures like Holmium Laser Enucleation (HoLEP) and GreenLight laser therapy use laser energy to remove or vaporize prostate tissue.
- These methods offer symptom improvement comparable to TURP but with shorter recovery times and less bleeding. Retreatment rates for GreenLight therapy are around 5.2%.
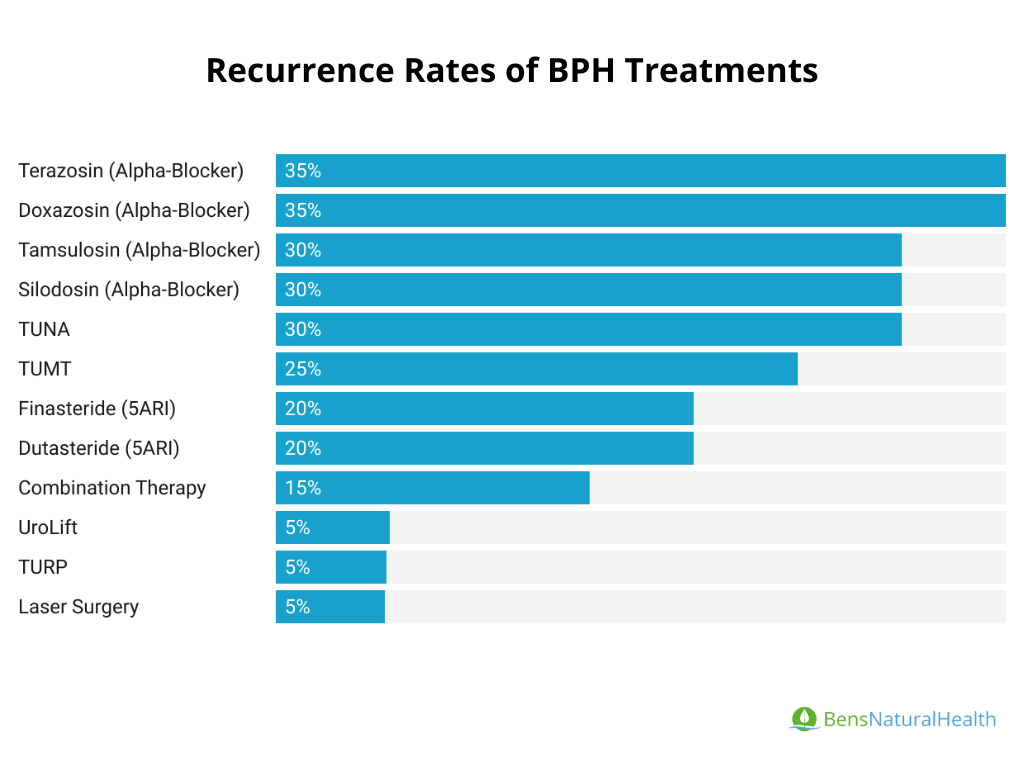
Recurrence Rates of BPH Post-Treatment
Medication Therapy: Patients on medications such as alpha-blockers or 5-alpha reductase inhibitors experience a 20–30% chance of symptom recurrence after discontinuation. Combination therapy lowers recurrence risk compared to monotherapy.
Minimally Invasive Treatments: TUMT and TUNA have higher recurrence rates than TURP, with the additional treatment required in approximately 20–30% of cases within five years.
Surgical Options: TURP and laser therapies show the lowest recurrence rates, with around 5% of patients requiring retreatment within five years.
BPH Complications and Hospitalization Statistics
Untreated Benign Prostatic Hyperplasia (BPH) can lead to several severe complications, highlighting the importance of timely diagnosis and management.
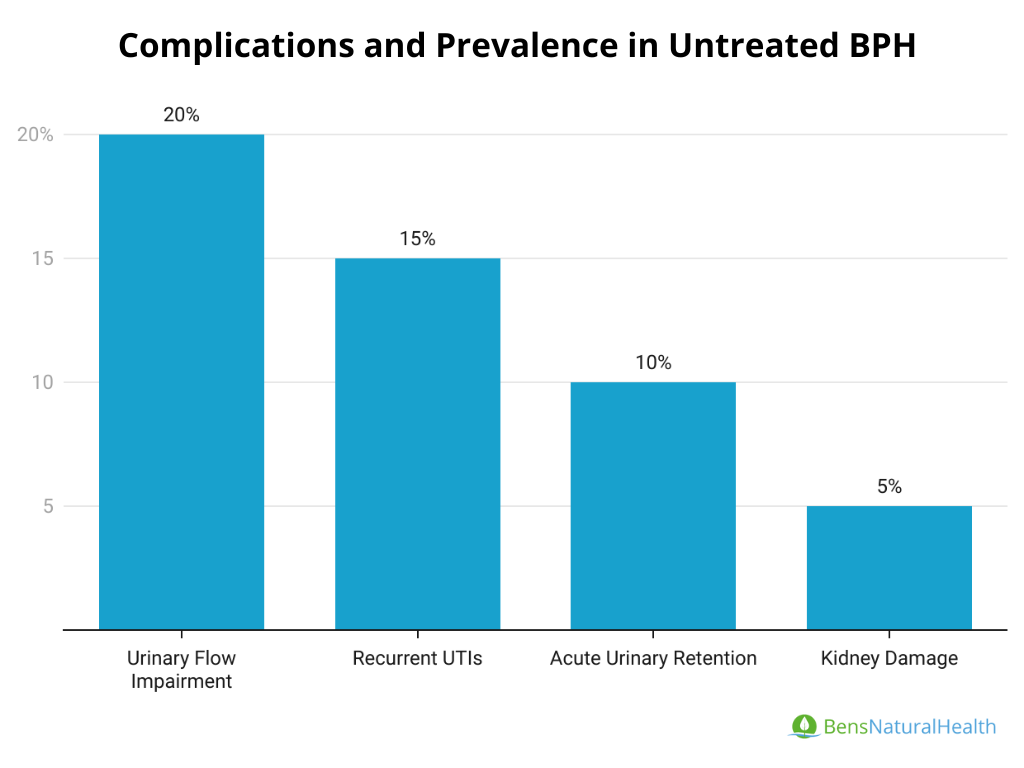
Complication Rates in Untreated BPH
- Urinary Retention: Acute urinary retention (AUR) occurs in 10-30% of untreated BPH cases, often requiring emergency catheterization or surgery. Chronic urinary retention can result in bladder overdistension, leading to irreversible damage to bladder functionality.
- Urinary Flow Impairment: Men with untreated BPH experience a gradual decline in urinary flow rates. The average peak flow rate improvement with treatment is 16-25%, which is notably absent in untreated cases.
- Increased Risk of Urinary Tract Infections (UTIs): The stagnant urine resulting from obstruction increases the likelihood of recurrent UTIs, impacting approximately 15-20% of men with severe BPH symptoms.
- Kidney Damage: Prolonged obstruction and high residual urine volumes can lead to hydronephrosis, a condition that causes kidney swelling and impairs kidney function. This complication, though less common, can become life-threatening if untreated.
BPH Mortality Rate Statistics
Benign prostatic hyperplasia (BPH) is a common condition among aging men, characterized by prostate enlargement leading to urinary symptoms. While BPH can significantly impact quality of life, it is generally not considered a direct cause of mortality.
BPH Date Rate in the U.S.
Benign prostatic hyperplasia (BPH) remains a non-lethal condition for most age groups. According to WHO mortality data, BPH-related deaths are exceedingly rare in younger populations and primarily occur in older age groups due to complications or associated conditions.
- The death rate has consistently ranged between 0.3 and 0.4 deaths per 100,000 males, indicating a favorable prognosis in BPH patients.
BPH Mortality Rate by Age Group
BPH mortality remains age-dependent, with negligible risks in younger populations and increasing risks in men aged 55 and older. Advanced age (75+) accounts for the majority of BPH-related deaths, reflecting the intersection of BPH progression and age-related health vulnerabilities.
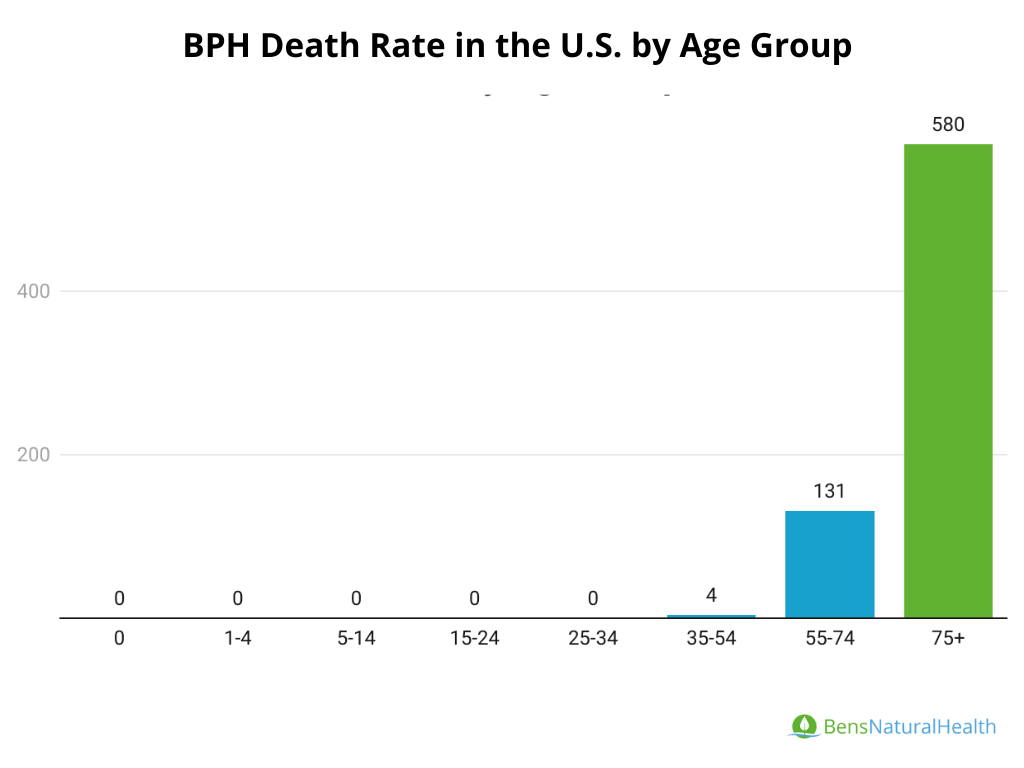
- Ages 0-34: There are no recorded deaths attributed to BPH in these age groups.
- Ages 35-54: A very low mortality rate is observed, with only 4 deaths recorded.
- Ages 55-74: Mortality rates increase significantly, with 131 deaths recorded, reflecting the higher prevalence and complications of BPH in this group.
- Ages 75+: This group exhibits the highest mortality, with 580 deaths reported, likely influenced by age-related comorbidities and advanced BPH complications.
BPH Death Rate in the U.S. by Year
The mortality rate for benign prostatic hyperplasia (BPH) has shown a gradual increase in recent years, according to WHO mortality data. Below is a summary of reported deaths among males attributed to BPH for the years 2012–2021:
- 2012: 519 deaths
- 2013: 558 deaths
- 2014: 547 deaths
- 2015: 571 deaths
- 2016: 642 deaths
- 2017: 619 deaths
- 2018: 578 deaths
- 2019: 636 deaths
- 2020: 707 deaths
- 2021: 715 deaths
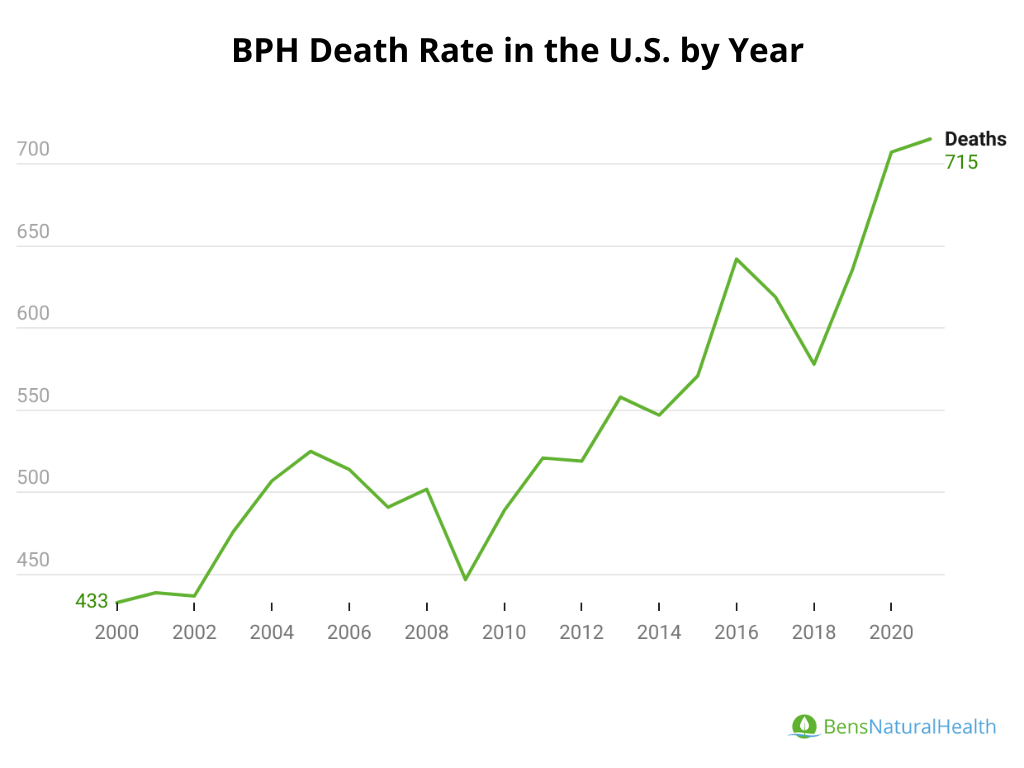
The gradual increase, with a notable jump between 2019 and 2020, may reflect broader health trends or reporting changes.
The peak in 2021 (715 deaths) represents a significant increase of approximately 37% compared to 2012 (519 deaths).
While BPH-related mortality is relatively low compared to other causes of death, the increasing trend suggests the need for continued attention to BPH management and prevention of complications, particularly in aging populations where the condition is most prevalent.
Trends in BPH Cause-Specific Mortality Across Selected Countries (2000–2021)
- United States of America (USA): Mortality from BPH was 715 deaths in 2021, reflecting a relatively stable trend from previous years.
- Mexico: Reported 1,017 deaths in 2021, showing an increase compared to earlier years.
- Brazil: Data unavailable for 2021, but 2020 showed 1,141 deaths, indicating a significantly high BPH mortality rate relative to other countries.
- Argentina: 52 deaths in 2021, demonstrating a consistently low mortality rate over the years.
- Colombia: Recorded 531 deaths in 2021, reflecting a gradual increase in recent years.
- Chile: 89 deaths in 2021, showing some fluctuation but remaining relatively low.
- Paraguay: 66 deaths in 2021, with slight variations compared to prior years.
Healthcare Costs Statistics on BPH
Direct Costs:
- Include diagnostic evaluations (e.g., PSA tests, ultrasounds), medications, minimally invasive therapies, and surgeries.
- In the U.S., annual direct costs for BPH management range between $1.1 billion and $2 billion, depending on the treatment type.
Indirect Costs:
- Indirect costs stem from lost productivity due to symptom-related disruptions, caregiving needs, and complications requiring hospitalization.
- Indirect costs are estimated to contribute an additional 25-30% to the overall economic burden of BPH.
Out-of-Pocket Costs for BPH Treatment by Insurance Coverage
- With Insurance:
- Patients with private insurance typically pay 10-20% of treatment costs for procedures like TURP or minimally invasive therapies, averaging $300–$500 per session.
- Prescription costs for BPH medications (e.g., alpha-blockers) are reduced significantly, with monthly co-pays ranging from $10 to $50 depending on the plan.
- Without Insurance:
- Out-of-pocket expenses for minimally invasive treatments range from $2,000 to $7,000 per session.
- Medications can cost between $50 and $150 monthly, while surgical interventions can exceed $10,000.
Quality of Life Impact Statistics for BPH Patients
Benign Prostatic Hyperplasia (BPH) significantly impacts the quality of life for affected men. Research shows the following:
- A study found that 12.45% of men with moderate to severe BPH symptoms reported poor quality of life using the International Prostate Symptom Score (IPSS) questionnaire
Comorbidities and BPH Statistics
BPH is often associated with several systemic comorbidities, which include:
- Hypertension: Studies indicate a higher prevalence of hypertension in men with BPH due to shared vascular and metabolic risk factors.
- Metabolic Syndrome: Men with BPH symptoms are more likely to present metabolic syndrome components, such as central obesity, dyslipidemia, and insulin resistance.
- Diabetes: Diabetes is a notable comorbidity in BPH patients, possibly due to inflammation, changes in urinary function, and vascular contributions to prostatic growth.
BPH and Mental Health Statistics
BPH not only affects physical health but also mental well-being:
- Anxiety and Depression: LUTS severity correlates strongly with increased scores for anxiety and depression, reflecting how persistent symptoms contribute to psychological strain.
- Chronic Sleep Disruption: Nocturia, a common symptom of BPH, leads to fragmented sleep, which is associated with fatigue, cognitive impairments, and mood disorders.
Future Predictions and Research Directions for BPH
Benign Prostatic Hyperplasia (BPH) is a common condition affecting aging men, with its global prevalence anticipated to increase due to demographic changes. Advancements in research and innovative treatments continue to improve management approaches and enhance patient outcomes.
Global Predictions for BPH
Rising Prevalence: Based on historical data, BPH cases globally are projected to exceed 90 million by 2030, increasing from 79 million cases in 2019 among men aged 60 and older. This growth is driven by population aging, lifestyle changes, and improved detection rates.
Historical growth (1990–2019) showed a 119.01% increase, with low-middle income regions experiencing the highest growth at 162.37%. Similar trends are expected to continue.
Regional Disparities:
- High-Prevalence Regions: China, India, and the United States will likely remain the top three contributors to global BPH cases.
- Emerging Hotspots: Eastern Europe, Central Latin America, and South Asia are expected to report increasing prevalence rates due to demographic shifts and healthcare access disparities.
Economic Impact: By 2030, the economic burden of BPH is projected to surpass $10 billion globally, factoring in both direct treatment costs and indirect losses from productivity and caregiving needs.
Research and Innovation: The focus on minimally invasive therapies and personalized medicine will grow, driven by the adoption of advanced surgical methods (e.g., HoLEP, UroLift) and novel drug combinations.
US Predictions for BPH
- Increasing Incidence: The number of men affected by BPH in the U.S. is projected to rise from 14 million in 2020 to over 18 million by 2030, with prevalence among men aged 51–60 exceeding 50% and 80% in men over 80.
- Age-Specific Trends: The 65–69 age group will continue to have the highest incidence rates, peaking at ~2,500 cases per 100,000 population, followed closely by men aged 75–79, where prevalence could reach ~30,000 per 100,000.
- Advanced Therapies: Utilization of advanced therapies like laser treatments and combination drugs is expected to grow by 20-25% annually, improving patient outcomes and reducing recurrence rates.
- Healthcare Costs: Out-of-pocket costs for uninsured patients could rise by 15-20% due to inflation and demand for advanced therapies, with surgical interventions potentially exceeding $15,000 per case by 2030.
- Genetic Research and Early Detection: Increasing investment in genetic research is expected to identify biomarkers for early detection and targeted therapies, improving outcomes for high-risk groups like those with a family history of BPH.
Research Methodology for BPH Statistics
This methodology ensures that our BPH statistics page is comprehensive, data-driven, and adheres to the highest standards of reliability and transparency.
Data Collection: To ensure accuracy and reliability, we collected data from reputable and trustworthy sources, including:
- Peer-reviewed research articles and clinical studies
- Public Databases and Reports: World Health Organization (WHO) Mortality Database, Prostate Drug Report 2021
- Expert Opinions and Guidelines: American Urological Association (AUA) Guidelines. Economic analyses by Saigal and Joyce on the costs of BPH in private healthcare sectors.
Data Analysis:
- We employed descriptive statistics to evaluate prevalence, incidence, and economic trends globally and regionally.
- Comparative Analysis was used to identify differences in prevalence rates across age groups, geographic regions, and healthcare systems.
- Trend Analysis allowed us to project future BPH cases and economic burdens using historical data from 1990 to 2019.
- We ensured consistency and accuracy by cross-referencing data from multiple sources, reconciling any discrepancies.
Expert Review: Urologists and medical researchers specializing in BPH reviewed the findings and interpretations to ensure alignment with current medical knowledge and practices. This step ensures that our insights are both accurate and clinically relevant.
Ethical Standards: We used publicly available and ethically sourced data, ensuring no personal or identifiable information was included. Adherence to strict ethical guidelines in handling data from clinical studies, registries, and global reports was maintained throughout.
Limitations:
- Variability in data collection methods across regions may introduce minor inconsistencies.
- Data lag from registries and limited access to emerging data may affect the representation of recent trends.
- Healthcare access and economic disparities in low-middle-income regions could impact the interpretation of prevalence and treatment statistics.
Ongoing Review and Updates: This page will be regularly updated with new data as it becomes available. We aim to include the latest research findings and expert feedback to ensure the continued accuracy and relevance of the information.
Conclusion
Benign Prostatic Hyperplasia (BPH) is a common condition affecting millions globally, with cases expected to rise due to aging populations. In the BPH statistics, we’ve highlighted the key trends, treatment advancements, and the importance of early detection. By staying informed and supporting ongoing research, we can improve the quality of life for those affected by BPH.